17%
%
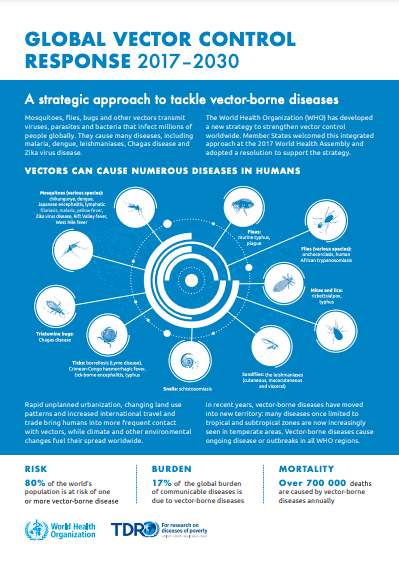
Vector-borne diseases account for more than 17% of all infectious diseases, causing more than 700,000 deaths annually.

Vector-borne diseases, including malaria, dengue, schistosomiasis, human African trypanosomiasis, leishmaniasis, Chagas disease, yellow fever, Japanese encephalitis and onchocerciasis, are strongly affected by climatic conditions such as temperature, rainfall and humidity. They account for more than 17% of all infectious diseases, causing more than 700,000 deaths annually.
Vector-borne diseases are highly sensitive to the environment, and climate change is affecting the distribution and transmission of many infectious diseases. The climatic suitability for the transmission of dengue increased by 11·5% for Aedes aegypti and 12·0% for Aedes albopictus from 1951–1960 to 2012–2021. The length of the transmission season for malaria increased by 31.3% and 13.8% in the highlands of the Americas and Africa, respectively, from 1951–1960 to 2012–2021.1 12022 Global Report of the Lancet Countdown In recent years, large outbreaks of emerging diseases such as Zika virus, Chikungunya and dengue have infected millions and overwhelmed health systems.
Vector-borne diseases account for more than 17% of all infectious diseases, causing more than 700,000 deaths annually.
Vector-borne diseases such as Chagas disease (transmitted by triatomine bugs), leishmaniasis (sandflies) and schistosomiasis (snails) affect hundreds of millions of people worldwide.
Vector borne diseases encompass a variety of illnesses that are caused via the spread of pathogens by living organisms known as vectors. These infectious diseases can be transmitted via vectors among humans (e.g., malaria, dengue), among animals (e.g., African swine fever, East Coast fever), or from animals to humans (e.g., Nipah virus disease). Many of these vectors are bloodsucking insects, and mosquitoes are the best known disease vector. Other vectors include ticks, flies, sandflies, fleas, triatomine bugs and some species of freshwater aquatic snails. 2 2WHO 2020 via UNDRR/ISC Hazard Information Profiles: Supplement to UNDRR-ISC Hazard Definition & Classification Review: Technical Report
View more hazard definitions in our glossary >
Vector-borne disease burden is highest in tropical and subtropical areas and disproportionately affects the poorest populations and those who lack access to health services.
Many vector-borne diseases were historically confined to distinct geographical areas, but have seen their range shift due to changing climate conditions, changing land use patterns, population movements and rapid and unplanned urbanization.
Increasing climate suitability for Aedes mosquitoes is contributing to the re-emergence of some of the world’s most deadly diseases. Over the past two decades, many important vector-borne diseases have re-emerged or spread to new parts of the world, including dengue, West Nile virus, and Zika virus. These diseases pose an increasingly wider threat to global public health, in terms of the number of people affected and their geographical spread.
The expansive re-emerging of vector-borne diseases such as zika and chikungunya has proven hard to control due to the lack of vaccines or specific treatments. The lack of access to health services or clean water for almost half of the world’s population is the main barrier to controlling the impacts of climate-sensitive diseases.
The health impacts of vector-borne diseases are vast, including impacting neurological function and causing severe morbidity. Vector-borne diseases can cause:
Vectors are living organisms that can transmit infectious pathogens between humans, or from animals to humans. Many of these vectors are bloodsucking insects, which ingest disease-producing microorganisms during a blood meal from an infected host (human or animal) and later transmit it into a new host, after the pathogen has replicated. Often, once a vector becomes infectious, they are capable of transmitting the pathogen for the rest of their life during each subsequent bite.3 3WHO Factsheet: Vector-borne diseases
Many vectors thrive under conditions where housing is poor, water is unsafe and environments are contaminated, so vector-borne diseases exact the heaviest toll on the poor and those with no or limited access to healthcare. Those with weakened immunity are also more vulnerable to the health impacts of vector-borne diseases.
Vulnerable populations include:
Vector-borne diseases are highly sensitive to climatic and environmental conditions. Temperature, rainfall and humidity affect the biology and ecology of vectors and hosts, and consequently impact disease transmission.
Rising global temperatures and changing weather patterns, including increased rainfall, are expected to alter transmission of many vector-borne diseases and in some areas increase the likelihood of disease.4 4Climate change and vector-borne diseases: a regional analysis. Githeko et al. 2000
Evidence has already shown that climate change has increased the climate suitability of disease transmission of malaria and dengue.5 52022 Global Report of the Lancet Countdown
Temperature
Low and high temperatures affect survival, development and activity level of the vector and the pathogen.
In general, higher temperatures tend to favour the transmission of vector-borne diseases such as malaria, dengue, Lyme disease and West Nile Fever.6 6Quantifying the effects of temperature on mosquito and parasite traits that determine the transmission potential of human malaria. Shapiro et al 2017;7 7A systematic review and meta-analysis of dengue risk with temperature change. Fan et al. 2015 8 8Effect of rising temperature on Lyme Disease: Ixodes scapularis population dynamics and Borrelia burgdoferi transmission and prevalence. Wallace et al. 2019 9 9Effects of temperature on emergence and seasonality of West Nile Virus in California. Hartley et al. 2012 The malaria parasite Plasmodium falciparum cannot replicate below 18ºC, nor can the Japanese encephalitis virus below 20ºC.10 10Climatic and geographic influences on arboviral infections and vectors. Mellow & Leake 2000
Warmer water temperatures shorten the time needed for mosquito larvae to mature, allowing them to produce more offspring during the transmission period.11 11Temperature-dependent development and survival rates of Culex quinquefasciatus and Aedes aegypti (Diptera: Culicidae). Rueda LM et al. 1990 Adult female mosquitoes can also digest blood faster and feed more often in warmer climates, increasing the intensity of disease transmission.12 12Temperature-dependent development and survival rates of Culex quinquefasciatus and Aedes aegypti (Diptera: Culicidae). Rueda LM et al. 1990 The disease-causing parasites and viruses may also complete their development in a shorter time at warmer temperatures, increasing the proportion of infective vectors.13 13Effects of environmental temperature on the vector competence of Aedes fowleri for Rift Valley fever virus. Turell MJ. 1989
In some areas, however, disease transmission may be reduced by climate change, due to temperatures that are too warm for parasite and vector survival.14 14Temperature-dependent development and survival rates of Culex quinquefasciatus and Aedes aegypti (Diptera: Culicidae). Rueda LM et al. 1990 For example, for the tsetse flies that transmit African trypanosomiasis, increased temperatures can lead to reductions in disease transmission.15 15Climate change and African trypanosomiasis vector populations in Zimbabwe’s Zambezi Valley: A mathematical modelling study. Lord et al. 2018.
Rainfall, Drought and Floods
Rainfall can determine the availability of breeding sites for insect vectors. Increased rainfall has the potential to increase the number of breeding sites for vectors, such as mosquitoes, ticks, snails, and increased reservoirs of disease such as rodents. Greater amounts of rainfall has been associated with increases in dengue and Japanese encephalitis transmission.16 16The impact of climate on Japanese encephalitis. Hsu et al 200817 17Climate change and vector-borne diseases: a regional analysis. Githeko et al. 2000
Drought can affect water storage and land use, affecting the habitat availability for the vector – particularly during weather extremes. For example, long-term drought may negatively impact tick populations that transmit Lyme disease.18 18Effects of climate and climate change on vectors and vector-borne diseases: Ticks are different. Ogden & Lindsay 2016.
Floods can also impact vector populations by destroying habitats, such as for blackflies that transmit onchocerciasis.19 19Potential effects of warmer worms and vectors on onchocerciasis transmission in West Africa. Cheke et al. 2015
Indirect Links
Climate and weather conditions can also exert indirect effects, through effects on the natural environment and on human behaviour.20 20Climate change and vector-borne diseases: what are the implications for public health research and policy? Campbell-Lendrum et al. 2015
Human-modified environments can create suitable habitats for vectors, including for mosquitoes that transmit dengue and yellow fever.21 21Land use influences mosquito communities and disease risk on remote tropical islands: A case study using a novel sampling technique. Steiger et al. 2016 22 22The dengue vector Aedes aegypti: what comes next. Jansen & Beebe, 2010 Human settlement patterns, land use changes, health seeking behaviour and vector control all interact with climate factors to ultimately determine disease transmission.
Early warning systems can be used in locations where there is a demonstrable relationship between vector-borne disease outbreaks and a climate factor. For example, in areas where there is a distinct rainy season that is associated with an increase in vector abundance, forecasting of rainy seasons can be used to anticipate the timing and location of peak cases. Temperature can also be used as an important indicator. Many successful climate-based early warning systems have been developed for malaria in Africa and for dengue fever in South-East Asia.23 23Using climate to predict infectious disease outbreaks: a review. WHO, 2004
Vulnerability mapping using geospatial data and remote sensing can provide a better understanding of where susceptible populations are located and can help target control activities. For example, vulnerability to dengue can be mapped by using a water-associated disease index approach.24 24Mapping Global Vulnerability to Dengue using the Water Associated Disease Index. Fullerton et al. 2014 Vulnerability and adaptation assessments (V&As) of vector-borne diseases can also help inform national adaptation strategies and other climate policies.25 25Protecting health from climate change: vulnerability and adaptation assessment. World Health Organization. 2013
Vector and case surveillance is also crucial for monitoring the distribution of vectors that may transmit diseases, as well as measuring the effectiveness of vector control interventions. If control and elimination targets for malaria and other vector-borne neglected tropical diseases are to be met over the 2020-2030 period, vector control interventions need to play an increasingly prominent role. Where used appropriately, vector control can be effective in disrupting transmission and reducing disease burden, especially for vector-borne diseases for which there is no vaccine, such as Zika, chikungunya, leishmaniasis and Chagas disease.
A number of interventions for vector control exist. Interventions should be selected based on the behaviour of the vector, its habitat, feeding preference and seasons, local epidemiology of the disease, human activity, such as irrigation, socioeconomic conditions of affected communities and the feasibility of applying interventions acceptable to the population, and may include:
Currently Featuring
Currently Featuring
Currently Featuring

Currently Featuring
Currently Featuring
Malaria is the biggest killer among the vector-borne diseases, but it is preventable and curable. In 2020, there were an estimated 241 million cases of malaria worldwide, with an estimated 627,000 deaths.
Climate patterns and weather events are important in determining the incidence and geographic range of malaria, through changes in human behaviour, effects on the pathogen (Plasmodium), on the vector (Anopheles), and on the capacity to control the disease.
Between 1951-1960 and 2014–2023, an extra 17.1% of the global land area became suitable for the transmission of P. falciparum; and an extra 21.8% for the transmission of P vivax.26 262024 Report of the Lancet Countdown
Every year, there are an estimated 219 million cases of malaria globally, resulting in more than 400,000 deaths.
Children aged under 5 years are the most vulnerable group affected by malaria; in 2018, they accounted for 67% (272,000) of all malaria deaths worldwide.
Malaria is a life-threatening disease caused by parasites that are transmitted to people through the bites of infected female Anopheles mosquitoes. It is preventable and curable. In 2020, there were an estimated 241 million cases of malaria worldwide, with an estimated 627,000 deaths.27 27WHO 2020 via UNDRR/ISC Hazard Information Profiles: Supplement to UNDRR-ISC Hazard Definition & Classification Review: Technical Report
View more hazard definitions in our glossary >
Malaria causes a febrile illness, with symptoms usually appearing 10-15 days after the infective mosquito bite. Symptoms generally include fever, headache and chills, but health impacts differ depending on the type of malaria.
P. falciparum malaria is most severe type of malaria, and can be fatal if not treated within 24 hours. Malaria mortality is highest among children under five years of age.31 31WHO World Malaria Report 2018 In endemic areas of transmission, malaria infections may be asymptomatic due to people developing partial immunity to the disease.32 32WHO Factsheet: Malaria
Uncomplicated malaria typically consists of a cold stage with chills and shivering, a hot stage of fever, headaches, vomiting and nausea, followed by a sweating stage that includes tiredness.
Complicated malaria can cause anaemia, respiratory distress, multiple organ failure, coma and seizures. Cerebral malaria is the most severe neurological complication caused by infection and can result in brain damage and long-term health impacts such as epilepsy, cerebral palsy, hearing, visual and intellectual impairment.33 33Severe neurological sequela and behaviour problems after cerebral malaria in Ugandan children. Idro et al. 2010
Malaria infection can cause low birth weight when women are infected during pregnancy. Malaria also has a considerable economic impact, through the costs of healthcare, days lost in education and decreased productivity.34 34Social implications of malaria and their relationships with poverty. Ricci et al 2012
Malaria is caused by Plasmodium parasites. The parasites are spread to people through the bites of infected female Anopheles mosquitoes, called “malaria vectors.” There are 5 parasite species that cause malaria in humans, and 2 of these species – P. falciparum and P. vivax – pose the greatest threat.
In endemic areas where malaria transmission occurs in regular long seasons, mortality rates are highest among children who have not yet developed immunity. In epidemic areas, transmission occurs in short seasons or epidemics, causing widespread severe mortality.
Malaria has devastating effects on children under the age of five, with 75% of deaths in Africa occurring in children.35 35Conquering the intolerable burden of malaria. III. Progress and perspectives. Breman et al. 2004 In 2018, they accounted for 67% (272 000) of all malaria deaths worldwide.
An individual’s general level of health and immunity is also a factor determining vulnerability to infection.
Vulnerable groups include:
Transmission depends on climatic conditions that may affect the number and survival of mosquitoes, such as rainfall patterns, temperature and humidity. In many places, transmission is seasonal, with the peak during and just after the rainy season. Malaria epidemics can occur when climate and other conditions suddenly favour transmission in areas where people have little or no immunity to malaria. They can also occur when people with low immunity move into areas with intense malaria transmission, for instance to find work, or as refugees.
Climate change is expected to increase malaria burden in the tropics and in highland regions as a result of increasing climate suitability. Malaria is likely to spread into regions that had previously seen little or no malaria transmission as a result of warmer temperatures, such as in the Africa highlands.
Vector control is the main way to prevent and reduce malaria transmission. If coverage of vector control interventions within a specific area is high enough, then a measure of protection will be conferred across the community. Two forms of vector control – insecticide-treated mosquito nets and indoor residual spraying – are effective in a wide range of circumstances.
From a climate services perspective, early warning, surveillance and risk and vulnerability mappings are useful tools to predict and manage outbreaks.
Early warning systems for malaria combine case surveillance, monitoring of meteorological data and long-range climate modelling in order to provide policymakers and health officials the time necessary to protect vulnerable populations. Where malaria control is limited, climate information can provide valuable information about the potential timing and distribution of malaria.36 36Early warning systems for Malaria in Africa: From blueprint to practice. Cox & Abeku. 2007 The most effective early warning systems for malaria provide forecasts with adequate lead of where and when an epidemic is likely to occur, predict the number of cases that could occur, or whether a pre-defined threshold will be exceeded, implement a response and also continually evaluate the system.37 37A stitch in time: improving public health early warning systems for extreme weather events. Ebi & Schmier 2005
Risk and vulnerability mapping can be a useful decision-support tool to identify transmission ‘hotpots’ most at risk of the health impacts of malaria that can be incorporated into intervention planning. For example, hotspots of vulnerability in Tanzania have been identified surrounding Lake Victoria.38 38Mapping malaria risk and vulnerability in the United Republic of Tanzania: a spatial explicit model. Hagenlocher & Castro. 2015
Surveillance of both malaria vectors and cases is key to inform effective vector control strategies, identify factors that may compromise vector control and reliably track the burden of malaria.



Dengue is emerging as a serious public health concern. It is the most rapidly spreading mosquito-borne viral disease, showing a 30-fold increase in global incidence over the past 50 years.39 39Impact of Dengue. WHO 2013. The number of dengue cases is increasing as the disease spreads to new areas including Europe and more explosive outbreaks are occurring, driven by the combination of development and globalization, unplanned urbanization, spread and mixing of strains of the virus, and increasing climate suitability.40 40The geographic distribution of dengue fever and the potential influence of global climate change. Van Kleef et al. 2010
The climatic suitability for the transmission of dengue by Aedes albopictus and Aedes aegypti increased by 46.3% and 10.7% respectively between 1951–1960 and 2014–2023. 41 412024 Report of the Lancet Countdown
An average dengue episode represents 18.9 lost days for non-fatal hospitalized patients, at an average cost of US$1,491.42 42WHO: Vector-borne diseases
More than 3.9 billion people in over 129 countries are at risk of contracting dengue, with an estimated 96 million symptomatic cases and an estimated 40,000 deaths every year.
Dengue is a mosquito-borne disease that is caused by a virus of the Flaviviridae family and transmitted by female mosquitoes mainly of the species Aedes aegypti and, to a lesser extent, A. albopictus.43 43WHO 2020 via UNDRR/ISC Hazard Information Profiles: Supplement to UNDRR-ISC Hazard Definition & Classification Review: Technical Report
View more hazard definitions in our glossary >
Dengue is endemic in more than 100 countries in Africa, the Americas, the Eastern Mediterranean, South-East Asia and the Western Pacific, and more than 50% of the world’s population is predicted to be at risk of dengue infection. Dengue transmission is ubiquitous year-round in the tropics, with the highest risk areas in the Americas and Asia, which bears 70% of the global burden of apparent infections.44 44Refining the global spatial limits of dengue virus transmission by evidence-based consensus. Brady et al. 2012
The primary dengue vector Aedes aegypti is common in urban environments in the tropics and sub-tropics, where the combination of abundant mosquito breeding sites and high densities of human populations support high rates of infection. Ae. albopictus is also common in tropical and sub-tropical areas.
Dengue causes a wide spectrum of disease that ranges from acute febrile illness to severe hemorrhagic manifestations. Dengue infection is often difficult to distinguish, as the vast majority of cases do not have symptoms, are self-managed and not reported. Recovery from infection by one serotype provides lifelong immunity against that particular dengue virus, and subsequent infections by other serotypes increases the risk of developing severe dengue.
The impact of dengue often goes beyond the immediate medical effects, as epidemics often occur in large cities, significantly impacting economic development due to medical costs and working days lost, placing a strain on health systems. The economic costs of endemic dengue for individual professional healthcare systems can exceed hundreds of millions of US$ annually.45 45Global cost of dengue in the professional healthcare system. Shepard, Halasa, Undurraga, 2014
The symptoms of classic dengue fever, also known as breakbone fever, typically appear 4-7 days after the infective mosquito bite, last for several days and can include:
Severe dengue, or dengue hemorrhagic fever, is a less common but potentially fatal complication of infection as a result of fluid accumulation, respiratory distress, severe bleeding and organ impairment.
Temperature is an important factor that determines the biting rate of Aedes mosquito and development of both the vector and virus, as well as survival and reproduction. The time it takes from ingesting the virus to actual transmission to a new host (called the extrinsic incubation period) is between 8-12 days when the ambient air temperature is between 25-28C.46 46Extrinsic Incubation Period of Dengue: Knowledge, Backlog, and Applications of Temperature Dependence. Tjaden, N.B., et al., 2013
High levels of precipitation, humidity, typhoons and El Nino events also influence dengue transmission, as these conditions can generate water pooling and subsequent mosquito breeding sites.47 47Influence of environmental conditions on asynchronous outbreaks of dengue disease and increasing vector population in Kaohsiung, Taiwan. Lai 2011 Drought can also contribute to dengue transmission as a result of human behaviour and increased storage of water in containers that provide the mosquito vectors with artificial breeding sites.48 48Ecological links between water storage behaviors and Aedes aegypti production: implications for dengue vector control in variable climate. Padmanabha et al. 2010 Mosquito eggs of Ae. albopictus are particularly resilient and can remain viable through the dry season, resisting desiccation.
Climate change models have predicted that the geographic ranges of Aedes mosquitoes that transmit dengue will expand and areas will become increasingly suitable for the mosquito life cycle, as well as dengue virus transmission.49 49Dengue in a changing climate. Ebi, K.L. & Nealon, J. 2016
In addition, many endemic countries where dengue is likely to spread further have underdeveloped health systems, increasing the potential for negative impacts upon health. Ae. albopictus, currently a secondary vector for dengue transmission, can survive in cooler temperatures so is likely to become a more significant vector as the climate warms, especially in Europe.50 50Global temperature constraints on Aedes aegypti and ae. Albopictus persistence and competence for dengue virus transmission. Brady et al. 2014 Over the last 2 decades, climate conditions have become more suitable for Ae. albopictus in areas such as central and northwestern Europe, but less suitable elsewhere such as in southern Spain.51 51Suitability of European climate for the Asian tiger mosquito Aedes albopictus: recent trends and future scenarios. Caminade et al. 2012
A changing climate may also affect dengue transmission through effects on human systems, such as water storage, land use and irrigation.52 52Dengue in a changing climate. Ebi, K.L. & Nealon, J. 2016
Control and elimination of Aedes mosquitoes that transmit dengue is extremely difficult because they can adapt to human environments and their populations often recover from natural disturbances such as drought or vector control measures. Given these challenges, there has been a focus on implementing an integrated approach by incorporating locally appropriate packages of vector control interventions alongside improved dengue surveillance and outbreak response.
Early-warning systems and forecasting for dengue outbreaks provides an opportunity to ensure the health impacts of dengue infection are reduced and the burden on healthcare systems reduced. A number of environmental parameters have been used to attempt to forecast dengue outbreaks, which include temperature, rainfall, hygienic parameters, socioeconomic factors.53 53Surveillance of dengue fever virus: a review of epidemiological models and early warning systems. V. Racloz, R. Ramsey, S. Tong, W. Hu. 2012 Climate variables that can successfully be used for predicting dengue outbreaks include temperature and relative humidity.54 54Climate and dengue transmission: evidence and implications. C.W. Morin, A.C. Comrie, K. Ernst. 2013
In Puerto Rico a system was developed that predicted dengue outbreaks with two week intervals and with a three week lead-time and predictions were based on daily temperatures, rainfall and water budgets.55 55Superensemble forecasts of dengue outbreaks. Yamana et al. 2016
More recently, a predictive model was developed to predict dengue outbreaks in Barbados.56 56Nonlinear and delayed impacts of climate on dengue risk in Barbados: A modelling study. Lowe, R. et al. 2018 Monthly dengue cases can be predicted by combining the impact of drought and rainfall, and optimal conditions for dengue transmission were shown to be periods of drought followed by warm temperatures and heavy rainfall 4-5 months later.
Mapping tools for dengue surveillance have been able to combine a range of factors that contribute to dengue transmission and allow for risk visualization for better surveillance and vector control.
Vaccination provides a promising way of mitigating against the health impacts of dengue. Use of the vaccine is currently targeted towards those living in dengue endemic areas, ranging from 9-45 years of age and who have had at least one documented dengue virus infection previously.
Vector population control, including introducing Wolbachia bacteria57 57Stable introduction of a life-shortening Wolbachia infection into the mosquito Aedes aegypti. McMeniman et al. 2009 to mosquitoes to reduce the number of females that live long enough to become infectious and transmit dengue. A number of other tools in the pipeline include the development of ‘molecular insecticides’,58 58Molecular mosquitocides. DeSimone JM which target at specific insect tissues and are protected from degradation, insect genetic engineering that reduces resultant larval survival and has suppressed mosquito populations has shown promising results in Malaysia.59 59Open field release of genetically engineered sterile male Aedes aegypti in Malaysia. Lacroix et al. 2012; Successful suppression of a field mosquito population by sustained release of engineered male mosquitoes. Harris et al. 2012
Biological control, such as the use of larvivorous fish that can control Aedes populations. In Cambodia, the School Dengue Project led by Malaria Consortium are engaging the community in dengue control, rearing guppies to be used on dengue control in water sources.60 60Efficacy and community effectiveness of larvivorous fish for dengue vector control. Han, et al. 2015
Environmental management to prevent mosquito breeding and community involvement in such management, such as waste management, clearing of discarded tyres and tins that could serve as mosquito breeding sites.61 61Community involvement in dengue vector control: Cluster randomised trial. Vanlerberghe et al. 2009 Container larvicide treatment and container removal is often recommended to ensure sustained management of Aedes larvae in areas of highly productive breeding.62 62Reducing costs and operational constraints of dengue vector control by targeting productive breeding places: A multi-country non-inferiority cluster randomized trial. Tun-Lin et al. 2009
Currently Featuring


Water-borne and sanitation-related diseases, such as cholera, typhoid and dysentery, are a major contributor to global disease burden and mortality. These diseases can be spread through drinking water and recreational water contact, with the highest burden in the poorest societies and in children under five years.
The risk of water-borne disease is likely to increase with climate change as heavy rainfall, storms and warmer sea temperatures favour the spread of water-borne pathogens.
The environmental suitability for Vibrio transmission reached a record high in 2023, with 88,348 km of coastline with waters suitable in 2023 – up by 14·8% from the previous record in 2018. 63 632024 Report of the Lancet Countdown
Every year, more than 3.4 million people die as a result of water-related diseases.
Diarrhoeal diseases are the second leading cause of death in children under five, killing more than 2,000 children per day.64 64Global Diarrhea Burden. Centers for Disease Control and Prevention 2013; Where and Why Are 10 Million Children Dying Every Year? Black et al. 2003
88% of child deaths from diarrhoeal disease cases are attributed to unsafe water conditions and poor hygiene.65 65Global Diarrhea Burden. Centers for Disease Control and Prevention 2013; Where and Why Are 10 Million Children Dying Every Year? Black et al. 2003
Waterborne diseases are those diseases that are transmitted by ingestion of contaminated water.66 66WHO 2012 via UNDRR/ISC Hazard Information Profiles: Supplement to UNDRR-ISC Hazard Definition & Classification Review: Technical Report
View more hazard definitions in our glossary >
The distribution of water-borne pathogens is widespread and varies from one country to another. Pathogens such as Vibrio cholerae and Hepatitis E virus are restricted to certain tropical countries whilst others, such as cryptosporidiosis and campylobacteriosis are widespread.
Water-borne diseases are typically associated with regions that lack adequate water, sanitation and hygiene and can be a particular problem following natural disasters such as flooding, earthquakes and storms.
In areas of high population density, outbreaks of water-borne diseases are common. Diarrhoea due to water-borne infections is a rare occurrence for those in developed countries, but widespread throughout the developing world. In Southeast Asia and Africa, diarrhea is responsible for as much as 8.5% and 7.7% of all deaths, respectively.
Water-borne diseases can cause a variety of illnesses, ranging from those without symptoms to those that can be life-threatening:
Exposure to water-borne pathogens, such as bacteria, viruses and various parasites, can occur through ingestion of contaminated water, incidental ingestion during recreational activities, or by direct contact with the eyes, ears or open wounds. These pathogens may include organisms that are transmitted in faeces and also those that naturally occur in aquatic systems.
Those living on low-lying islands, such as Pacific Islands, Kiribati, Tuvalu and Vanuatu, which are vulnerable to frequent flooding events;
Climate primarily impacts water-borne disease through the contamination of water supplies.
Climate change is expected to increase the frequency and intensity of extreme weather events, such as flooding, droughts and storms, increasing water-borne disease risk.
Rainfall and flooding
In tropical regions, diarrhoeal diseases typically peak during the rainy season when water supplies are easily contaminated.67 67Environmental health engineering in the tropics: an introductory text. Cairncross & Feachem, 1993 Flooding in particular has been associated with water-borne disease outbreaks such as typhoid, rotavirus, leptospirosis because of water supply contamination from mixing of drinking and waste waters.68 68Risk factors for typhoid and paratyphoid fever in Jakarta, Indonesia. Vollaard et al 2004; Rotavirus-associated diarrhea in rural Bangladesh: Two-year study of incidence and serotype distribution. Fun et al 1991; Population-based case-control investigation of risk factors for leptospirosis during an urban epidemic. Sarkar U. et al. 2002
Rainfall affects the transport, survival and transmission of water-borne pathogens. Heavy rain events can flush pathogens from surrounding areas into streams or lakes, contaminate water treatment plants and distribution systems, and place excessive demand on sewage treatment plants.69 69Microbial load of drinking water reservoir tributaries during extreme rainfall and runoff. Kistemann et al. 2002;
Effects of weather and river flow on cryptosporidiosis. Lake et al. 2005;
Climate and waterborne disease outbreaks. Rose et al. 2000 Infiltration of Cryptosporidium into drinking water reservoirs is a particular problem, since this bacteria is resistant to chlorination treatment. Rainfall events can also flush organic matter and microbial nutrients into water distribution systems, and this can promote the growth of water-borne pathogens.
Drought
Drought events can also often lead to outbreaks of water-borne disease, due to lack of adequate water supplies for sanitation and hygiene.
Temperature
Temperature can also affect water-borne diseases, as it directly influences the survival, growth and persistence of water-borne pathogens.70 70Climate change and infectious diseases in Europe. Semenza and Menne 2009 Infections of Salmonella and Campylobacter show distinct seasonality, with higher disease rates at warmer temperatures during the summer months in places such as the US.71 71Enterovirus surveillance – United States, 1970-2005. Khetsuriani et al. 2006 In the Arctic, enteric disease risk is linked to temperature-related melting of permafrost which hastens transport of sewage into groundwater and drinking water sources.72 72Drinking water and potential threats to human health in Nunavik: adaptation strategies under climate change conditions. Martin et al. 2007 However, survival of some pathogens may be reduced at higher temperatures.
In many Pacific island countries, climate change is likely to exacerbate diarrheal illness due to increases in the extremes of rainfall and warmer temperatures.73 73The influence of climate variation and change on diarrheal disease in the Pacific Islands. Singh, R.B. et al. 2001
Other factors
In response to warming sea-surface temperatures, concentrations of water-borne pathogens such as Vibrio are expected to increase.74 74Effects of global climate on infectious disease: The cholera model. Lipp, E.K. et al. 2002;
Relationship between rainfall and beach bacterial concentrations on Santa Monica Bay beaches. Ackerman, D. & Weisberg, S. 2003
Altered seasonal patterns due to climate change, including lengthening of spring and summer seasons in the northern hemisphere, may create a longer transmission season for water-borne pathogens as suitable climate conditions for disease transmission persist for longer.75 75Knowledge mapping for climate change and food- and waterborne diseases. Semenza 2012
In addition, extended seasons for agricultural and leisure activities may also provide increased opportunities for exposure to water-borne pathogens.
It is estimated that 94% of diarrheal cases are preventable.76 76Combating Waterborne Disease at the Household Level. WHO. 2007 Modifications to the environment, through interventions to increase the availability of clean water and improve sanitation and hygiene, is the most effective way to tackle water-borne diseases. Diarrhoeal incidence can be reduced by 25% through improving water supply, 32% by improving sanitation, 45% through hand washing, and by 39% via household water treatment and safe storage.77 77Water, Sanitation, and hygiene interventions to reduce diarrhoea in less developed countries: a systematic review and meta-analysis. Fewtrell et al. 2005
Surveillance of water-borne diseases is critical to health impact management. Detection, recording and reporting helps authorities to recognise outbreaks, monitor interventions and provide rapid alerts of disease outbreaks.78 78Cryptosporidiosis surveillance and water-borne outbreaks in Europe. Semenza & Nicholas, 2007 Surveillance also enables for the identification of patterns in places or sources of infection or the predominant causal agents of outbreaks. For example, Norway’s national web-based outbreak rapid alert system has proved useful for analyzing trends in disease outbreaks, the occurrence of pathogens causing infections and the predominant routes of transmission.79 79The national webbased outbreak rapid alert system in Norway: eight years of experience, 2006–2013. Guzman-Herrador et al. 2016
Microbial testing of water samples can aid in detecting the causative agent can also help confirm the source of the outbreak.
Upgrading of water treatment and distribution systems can ensure systems are more robust and prepared for extreme weather events, such as flooding, which may overwhelm treatment and distribution systems.80 80Water distribution system and diarrheal disease transmission: A case study of Uzbekistan. Semenza et al. 1998
Household water sanitation to ensure sanitary sewage disposal, safe water piping materials and storage.
Augmenting sewage system storage capacity in order to minimize wet weather discharges can help reduce overflow volumes during extreme rainfall events.81 81Combined sewer overflow emissions to bathing waters in Portugal: How to reduce in densely urbanised areas? David & Matos 2005
Improved hygiene practices such as discouragement of open defecation, hand washing and creation of pop up facilities during natural disasters and population displacements.
Point-of-use disinfection using bleach solutions, encouraging boiling of water, and simple pot filters can be low-cost options of ensuring vulnerable populations have access to safe drinking water at the household level. Other low cost techniques include solar disinfection and chlorination of water sources.
Vaccination is available for some water-borne diseases, such as rotavirus, cholera, typhoid, enterotoxigenic E. coli and Shigella.
Serosurveillance of cases of water-borne diseases, for example has been developed for Salmonella spp, can provide data on asymptomatic infections and can give an indication of the true burden of disease as some infections are not notified or reported. Integrated surveillance can also help attribute infections to sources and reservoirs of water-borne pathogens.


Cholera is one of the main threats to health in developing countries, and is associated with seasonal climate conditions, natural disasters, poor water, sanitation and hygiene, and civil conflict.
An estimated 2.9 million Cholera cases and 95,000 deaths occur each year globally.82 82CDC. Cholera - Vibrio cholerae infection
Up to 80% of cases of cholera can be successfully treated with oral rehydration solution.83 83Updated global burden of cholera in endemic countries. Ali, M. et al. 2015
Cholera is an acute diarrhoeal infection caused by ingestion of food or water contaminated with the bacterium Vibrio cholerae. Cholera remains a global threat to public health.84 84WHO 2019 via UNDRR/ISC Hazard Information Profiles: Supplement to UNDRR-ISC Hazard Definition & Classification Review: Technical Report
View more hazard definitions in our glossary >
Cholera is endemic in 50 countries, including India, Ethiopia and Bangladesh, and can be found in virtually any coastal water body, especially in the tropics and subtropics. Sub-Saharan Africa accounts for around 60% and Southeast Asia 29% of the global burden of cholera cases.
The main regions of cholera endemicity include the coasts surrounding the Bay of Bengal, both Bangladesh and the Indian subcontinent, and coastal Latin America. Cholera frequently re-emerges during natural disasters, civil unrest, and in the breakdown of public health measures, for example during the Rwandan crisis in 1994 and in 2010 following earthquakes in Haiti.85 85The 2010 cholera outbreak in Haiti: How science solved a controversy. Orata et al 2014
In the US Gulf Coast and in Australia, outbreaks are often caused by the consumption of raw or improperly cooked shellfish contaminated with cholera bacteria.86 86Bergey’s manual of determinative bacteriology, 9th ed. Holt et al. 1994
Cholera is a highly contagious acute bacterial infection of the intestine. The infection is often mild and without symptoms but can cause acute diarrhea. In approximately 10% of infected people it can cause severe disease, which manifests as profuse watery diarrhea, vomiting and leg cramps. Rapid loss of body fluids as a result can lead to life threatening dehydration and shock.
Cholera is a water-borne disease caused by the bacterial pathogen Vibrio cholerae, which inhabits brackish water. Cholera may be transmitted by drinking water or by environmental exposure in seawater and seafood. In an epidemic, the main source of contamination is usually the faeces of an infected person that contaminates water and/or food. The disease can spread rapidly in areas with inadequate sewage treatment and drinking water.
Individuals living in areas of high population density, with unsafe sources of drinking water, poor sanitation and inadequate hygiene are at a greater risk of cholera infection. In addition, those in areas prone to natural disasters, such as flooding storms and earthquakes, are also vulnerable to cholera outbreaks as a result of compromised water, sanitation and hygiene following a disaster.
The cholera pathogen is strongly influenced by factors such as water temperature, pH and salinity.87 87Occurrence and distribution of the human pathogen Vibrio vulnificus in a subtropical Gulf of Mexico estuary. Lipp et al. 2001; Influence of salinity and organic nutrient concentration on survival and growth of Vibrio cholerae in aquatic microcosms. Singleton et al. 1982 Where cholera is endemic there is a robust relationship between warmer temperatures and the disease.
Cholera is also influenced by heavy rainfall and flooding events which promote the transmission of pathogens when sanitation and hygiene is compromised and there is not secure disposal of faecal waste.88 88Severe cholera outbreak following floods in a northern district of West Bengal. Sur, D. et al. 2000;
Review of reported cholera outbreaks worldwide, 1995-2005. Griffith, D.C. et al. 2006 Rainfall can also affect cholera incidence through its effects on nutrient concentrations, salinity and pH of water resources that impact bacterial survival.89 89Effects of global climate on infectious disease: the cholera model. Lipp, Huq, Colwell, 2002
Extreme weather events, such as hurricanes, typhoons can disrupt water systems, resulting in the mixing of drinking and waste waters, which increase the risk of cholera infection.90 90Atlas of Health and Climate. WHO / WMO 2012 The influence of El Nino events in Asia and South America also impact on cholera transmission, as more favourable climate conditions such as warmer sea-surface temperatures increase the observed incidences of cholera in these regions.91 91Climate and infectious disease: use of remote sensing for detection of Vibrio cholerae by indirect measurement. Lobitz et al. 2000; Cholera dynamics and El‐Niño‐Southern Oscillation. Pascual et al. 2000;
Cholera incidence and El‐Niño‐related higher ambient temperature. Speelmon et al. 2000
Warmer temperatures may increase the suitability for environmental reservoirs of the cholera pathogen, although temperatures that are too warm may negatively impact upon the survival of the pathogen.92 92Survival of Vibrio cholerae O139 Synonym Bengal in water from a river. Okitsu, et al. 1994 Despite this, predictions have shown climate change is likely to increase cholera incidence,93 93The effect of climate change on cholera disease: The road ahead using artificial neural network. Asadgol, Z. et al. 2019 and the percentage of coastal area suitable for Vibrio infections has increased by 31% in the Baltic coastline and by 29% in the northeastern coastline of the USA has already been demonstrated.94 94The 2019 report of The Lancet Countdown on health and climate change: ensuring that the health of a child born today is not defined by a changing climate. Watts, N. et al. 2019 The number of days per year suitable for Vibrio has also increased in Baltic and globally the environmental suitability for coastal V. cholerae has increased by 9.9%.
Sea-level rise that accompanies climate will also increase the risk of cholera, due to greater saltwater intrusion in inland areas, increasing levels of cholera bacteria.95 95Effects of global climate on infectious disease: the cholera model. Lipp, Huq, Colwell, 2002


Billions of people are at risk of food-borne diseases, which encompass a wide spectrum of illnesses and are a growing public health problem worldwide. Contaminated food causes 600 million people worldwide to fall ill every year.
Unsafe food containing harmful bacteria, viruses, parasites or chemical substances can cause more than 200 different diseases.100 100WHO: Food safety
Unsafe food causes 600 million cases of foodborne diseases and 420,000 deaths each year worldwide.101 101WHO: Estimating the burden of foodborne diseases
30% of foodborne deaths occur among children under 5 years of age.102 102WHO: Estimating the burden of foodborne diseases
Diarrhoeal diseases are the most common illnesses resulting from the consumption of contaminated food, causing 550 million people to fall ill and 230,000 deaths every year.103 103WHO: Food safety factsheet
Food-borne diseases are transmitted by consumption of contaminated biological food and drink, These diseases are caused by eating food contaminated with bacteria, viruses, parasites or chemical substances.104 104WHO via UNDRR/ISC Hazard Information Profiles: Supplement to UNDRR-ISC Hazard Definition & Classification Review: Technical Report
View more hazard definitions in our glossary >
Food-borne diseases occur everywhere. The types, severity and impacts of these illnesses are diverse across regions, countries and communities. Some food-borne diseases are particularly in areas with compromised sanitation and hygiene systems, and where food is not safely prepared. The highest burden of food-borne disease occurs in Africa, followed by South-East Asia.105 105WHO: Estimating the burden of foodborne diseases In many tropical countries, the climate favours the proliferation of pests and naturally occurring toxins, and the risk of contracting parasitic diseases.
The impacts of food-borne diseases range from mild and self-limiting to debilitating and life-threatening, leading to long periods of absenteeism and premature death. Gastrointestinal problems are the most common health impacts of foodborne diseases and other serious consequences include kidney failure, and neurological disorders.
Only a fraction of people who become sick from food seek medical care, and certain chronic conditions such as cancer, kidney or liver failure that result from contaminated food appear long after the ingestion of the food and the causal links are never made.
Unsafe food is also linked to nutrition and food security, and food-borne disease can create a vicious cycle of disease and malnutrition, particularly affecting infants, young children, elderly and the sick.
Symptoms of food-borne diseases may include:
Food-borne diseases can result from ingestion of food contaminated with microorganisms, such as bacteria, viruses and parasites, or chemicals. Food contamination may occur at any stage in the process from food production to consumption, and can result from environmental contamination, including pollution of water, soil or air.
Illnesses from seafood can result from biotoxins in marine environments that contaminate food sources. The most frequent causes of food-borne illness are diarrheal disease agents, such as norovirus and Campylobacter spp. Food-borne diarrheal disease agents cause the highest numbers of deaths worldwide, particularly Salmonella, hepatitis A and aflatoxin.
Weather and climate can influence the replication, transport and dissemination of microbial agents that cause food-borne diseases.
Heavy rains and flooding can flush disease-causing microorganisms and toxic chemicals into watersheds, coastal zones and cropland where they may contaminate food sources.
Elevated temperatures as a result of climate change will accelerate the replication cycles of food-borne pathogens such as Salmonella and Campylobacter, and extended summer seasons may increase the opportunities for deficiencies in food handling.106 106Knowledge mapping for climate change and food- and waterborne diseases. Semenza, 2012; The Effect of Temperature on Food Poisoning: A Time Series Analysis of Salmonellosis in 10 European Populations. Kovats et al. 2004.
The extended growing season may also encourage greater use of outdoor pasture and increase the risk of pathogen transmission from the environment.
Warmer sea surface temperatures and changing weather patterns may increase the risk of marine biotoxin accumulation and seafood illnesses from Vibrio spp.
Increased frequency and intensity of extreme weather events, such as droughts, storms and floods may increase the risk of contamination events and compromise adequate food storage.
Ciguatera poisoning is the most frequently reported seafood-toxin illness in the world, with as many as 50,000 cases reported annually.107 107WHO. Ciguatera Fish Poisoning factsheet. It is caused by ingestion of contaminated reef fish such as barracuda, grouper and snapper, and can result in debilitating neurological symptoms that persist with varying severity for weeks to months after contamination.
Ciguatera is endemic in tropical and subtropical regions of the Pacific, Indian Ocean and Caribbean, with isolated outbreaks in temperate areas such as Europe and North America and new areas occurring as a result of increasing travel and import of susceptible fish.108 108Ciguatera poisoning: a global issue with common management problems. Ting & Brown, 2001
The prevalence of ciguatera is associated with warm sea surface temperatures, as well as El Nino events.109 109Ciguatera fish poisoning and sea surface temperatures in the Caribbean Sea and the West Indies. Tester et al. 2010 Climate change is projected to expand the range of suitable habitat for the algae that cause ciguatera, and increases in storm frequency may also contribute to wider spread.110 110 Impacts of climate variability and future climate change on harmful algal blooms and human health. Moore et al. 2008; Ciguatera. Swift AE, Swift TR. 1993 Evidence suggests that warming of temperatures between 2.5-3.5°C in the Caribbean Sea could increase the incidence of ciguatera by 200-400% in the United States.111 111Ciguatera fish poisoning and climate change: analysis of National Poison Center Data in the United States, 2001-2011. Gingold, Strickland, Hess, 2014
Monitoring of toxic algae around the world can provide early warning to help protect against the health impacts of toxic marine species. Currently many attempts are being made to develop specific forecasting systems for ciguatera, which is being made possible through breakthroughs in identification of toxic dinoflagellate species.
Food-borne diseases are preventable and can be controlled through an effective food safety system that considers hazards from production to consumption. Food safety can be achieved through coordinated action across multiple sectors to build strong and resilient national food safety systems and provide consumers with tools to make safe food choices.
Expansion of the international food trade means that food contaminated in one country can cause disease in other countries, and trade restrictions are often applied to countries identified as a source of contaminated food.
Many food-borne diseases often go undetected and under-reported so there is a great need for improving epidemiological surveillance. Surveillance of food-borne disease through systematic recording, analysis and interpretation of data about illness in individuals can help detect outbreaks, monitor trends and evaluate interventions. Surveillance data for plant, animal and human systems should be integrated into a One Health approach to maximise the potential of identifying any new threats.
Rapid risk assessment of acute public health events can provide the basis for action to manage and reduce the negative consequences of food-borne outbreaks and ensure timely control measures are taken. By estimating the level of exposure to the hazard in the community, the likelihood of spread, as well as community factors that may affect the health outcomes of food-borne outbreaks, such as the levels of malnutrition in the affected community, authorities can identify an event which might become a public health concern.
Improved biosecurity measures to minimise the risk of contamination.
Improved food hygiene practices and safety, including education on using clean water to wash cooking equipment, and policy changes such as incorporating street food into food safety laws. Health promotion and food safety campaigns to inform, educate and empower people may also help reduce individual risk.
Improved wastewater management and capacity so that systems are not overwhelmed during extreme weather events such as floods.


Currently Featuring

Currently Featuring
Air-borne diseases, including influenza, measles and tuberculosis, affect millions of people every year around the world. Environmental conditions influence transmission of air-borne diseases directly through changing humidity, temperatures and wind patterns, and indirectly through impacting the movement of people.
Tuberculosis (TB) infection is extremely common: an estimated one-quarter of the world’s population is infected, with 10 million people falling ill with TB yearly. Despite being a preventable and curable disease, 1.5 million people die from TB each year – making it the world’s top infectious killer. People with TB infection risk developing TB disease and this risk depends on multiple factors, the most important being the state of their immune system.
Measles is another highly contagious viral disease. It remains an important cause of death among young children globally, despite the availability of a safe and effective vaccine.
1.5 million people died from tuberculosis in 2018.
Influenza results in 3-5 million cases of severe illness every year worldwide..
99% of deaths in children under 5 years of age from seasonal influenza epidemics occur in developing countries.112 112Global burden of respiratory infections due to seasonal influenza in young children: a systematic review and meta-analysis. Nair H, Abdullah Brooks W, Katz M et al. Lancet 2011
Airborne transmission of infectious agents refers to the transmission of disease caused by dissemination of very small droplets that remain infectious when suspended in air over long distance and time113 113WHO 2020 via UNDRR/ISC Hazard Information Profiles: Supplement to UNDRR-ISC Hazard Definition & Classification Review: Technical Report
View more hazard definitions in our glossary >
Many air-borne diseases, like influenza, are extremely common and circulate all around the world. Other air-borne diseases are restricted to certain areas, such as severe acute respiratory syndrome in China and Middle East Respiratory Syndrome.
Dense urban settlements have been linked to airborne disease transmission. For instance, households with poor ventilation, poor sanitation, or crowding promote transmission of tuberculosis.
Most of the people who fall ill with TB live in low- and middle-income countries, but TB is present all over the world. About half of all people with TB can be found in 8 countries: Bangladesh, China, India, Indonesia, Nigeria, Pakistan, Philippines and South Africa.
While vaccination has drastically reduced global measles deaths — a 73% drop between 2000-2018 worldwide — measles is still common in many developing countries, particularly in parts of Africa and Asia. More than 140,000 people died from measles in 2018. The overwhelming majority (more than 95%) of measles deaths occur in countries with low per capita incomes and weak health infrastructures.
Many air-borne diseases are very common and can have mild symptoms, however severe symptoms can manifest in vulnerable persons and those with an existing chronic illness. Some diseases, such as measles, are highly contagious and can result in death.
Symptoms of air-borne diseases may include:
Air-borne diseases are spread via the air from an infected person via coughing, sneezing, talking and close contact. Pathogens that can be transmitted include bacteria, viruses and fungi and they may be spread in aerosols, dusts or liquids. These aerosols can be generated from bodily secretions of an infected person, or biological wastes such as those accumulated in lofts and caves. Infected aerosols can remain suspended in air currents and travel considerable distances to transmit diseases.
Climatic factors including humidity, temperature and wind can affect how pathogens are carried in the air. For example, respiratory syncytial virus (RSV) exhibits epidemic peaks in the winter in temperate climates.114 114The relationship of meteorological conditions to the epidemic activity of respiratory syncytial virus. Yusuf et al. 2007
Wind is a key factor that affects air-borne pathogen transmission. Viral pathogen transport and survival is increased during dust storms as dust particles can act as transport vehicles for the pathogens.115 115Ambient influenza and avian influenza virus during dust storm days and background days. Chen, 2010; Atmospheric movement of microorganisms in clouds of desert dust and implications for human health. D.W. Griffin, 2007; Transport of microorganisms to Israel during Saharan dust events. Schlesinger, Mamane, Grishkan, 2006 The Influenza virus can be transported from Asia to the Americas in winter months by prevailing wind over the Pacific.116 116The Pacific ENSO Applications Center and the 1997–98 ENSO Warm Event in the US-affiliated Micronesian Islands: Minimizing Impacts Through Rainfall Forecasts and Hazard Mitigation. Hamnett, Anderson, Guard. 1999
In some instances, climate change may shorten the transmission season for airborne diseases such as RSV and influenza, but RSV epidemics may be more severe due to increases in humidity.117 117Climate change and the end of the respiratory syncytial virus season. Donaldson 2006; Epidemic dynamics of respiratory syncytial virus in current and future climates. Baker et al. 2019
Air-borne diseases often exhibit seasonal transmission in the Northern Hemisphere, such as influenza.118 118African dust in the Caribbean atmosphere: microbiology and public health. Griffin et al.. 2001 Cold temperatures and low humidity are posited to be favourable for transmission of influenza, and humidity may also affect the survival of aerosolized virus particles.119 119Climatological and geographical impacts on global pandemic of influenza A (H1N1). Xu et al. 2014; Absolute humidity modulates influenza survival, transmission, and seasonality. J. Shaman, M. Kohn, 2009; Influenza virus transmission is dependent on relative humidity and temperature. A.C. Lowen, S. Mubareka, J. Steel, P. Palese. 2007; African dust in the Caribbean atmosphere: microbiology and public health. Griffin, D. W., V. Garrison, and E. A. Shinn. 2001
Heatwaves and other extreme weather may contribute to increased morbidity and mortality from air-borne diseases.120 120Climate change and human health in China. H. Kan. 2011 Increased air temperature and wind speeds may decrease transmission of air-borne pathogens.121 121Climate change effects on airborne pathogenic bioaerosol concentrations: a scenario analysis. Van Leuken, J.P.G. et al. 2016
Indirect effects, such as population displacements resulting from an increased frequency and severity of extreme weather events may bring people into contact and create suitable conditions for air-borne disease transmission.
Air-borne diseases spread easily, and are difficult to prevent. Risk management and mitigation strategies include:


Meningococcal meningitis is a severe infectious disease of the meninges, a thin layer around the brain and spinal cord. It is a devastating disease and remains a major public health challenge.
Future temperature increases associated with climate change have the potential to increase the incidence of meningitis, due to a lengthening of the seasonal transmission period. In addition, the increased frequency and intensity of droughts, and dust storms predicted to occur with climate change will also provide more suitable climate conditions to facilitate meningitis transmission.
Dust and the Wind: Climate and Meningitis In Niger from IRI on Vimeo.
The largest recorded epidemic occurred in 1996-1997 and caused 250,000 cases and 25,000 deaths.
Meningococcal meningitis fatality is up to 50% when untreated.122 122WHO. Meningococcal meningitis factsheet
Approximately 30,000 cases are reported in the sub-Saharan Africa “meningitis belt” each year.123 123WHO. Meningococcal meningitis factsheet
Meningococcal meningitis is a bacterial form of meningitis, a serious infection of the thin lining that surrounds the brain and spinal cord, that is caused by the bacterium Neisseria meningitidis. Meningococcal meningitis has the potential to cause large-scale epidemics and is observed worldwide124 124WHO 2018 via UNDRR/ISC Hazard Information Profiles: Supplement to UNDRR-ISC Hazard Definition & Classification Review: Technical Report
Meningitis is observed worldwide, but the majority of burden occurs in sub-Saharan Africa in an area called the “Meningitis Belt” that is regularly hit by epidemics during the dry season, from December to May.125 125TITLE
The health impacts of meningitis can be severe, with case fatality ranging between 10-15%.126 126Meningococcal carriage in the African Meningitis Belt. Trotter CL, Greenwood BM, 2007 Symptoms can include:
The disease is transmitted from person-to-person through droplets of respiratory or throat secretions. Close and prolonged contact, such as kissing, sneezing and coughing can facilitate disease spread.
Several microorganisms can cause meningitis. The bacterium with the greatest epidemic potential is Neisseria meningitidis. There are six serogroups of N. meningitidis which cause meningococcal disease.
The disease can be caused by many different pathogens including bacteria, fungi or viruses, but the highest global burden is seen with bacterial meningitis.
The disease can occur as sporadic cases, in small clusters or huge epidemics. A significant proportion of the global population carries the bacteria asymptomatically in the nose and throat, and never develops the invasive disease.
Meningococcal meningitis can affect anyone, but mainly affects babies and young children. The risk of acquiring the disease also increases with age. Those living in poverty and in overcrowded conditions, which facilitate disease transmission, are also vulnerable.
There is a clear seasonal pattern of meningitis cases in the meningitis belt that corresponds to the period of the year when there are increases in dust concentrations, as well as reductions in humidity levels and dry winter winds.128 128Environmental risk and meningitis epidemics in Africa. Molesworth et al. 2003; Climate drives the meningitis epidemics onset in West Africa. Sultan et al. 2005
Dry hot dusty air irritates respiratory mucosa, facilitating invasion of the bacteria which can more easily penetrate injured mucosal membranes and access the bloodstream and travel to the meninges. Incidence of the disease drops dramatically during the rainy season.
In countries outside Africa, meningitis also exhibits a similar seasonal pattern, with peak cases occurring during dry winter months.129 129Update on meningococcal disease with emphasis on pathogenesis and clinical management. van Deuren et al. 2000; Seasonal variation in meningococcal disease in Denmark: relation to age and meningococcal phenotype. Jensen et al. 2003;
Forty years of meningococcal disease in Israel: 1951-1990. Block et al. 1993; Do environmental factors influence the occurrence of acute meningitis in industrialized countries? An epidemic of varying aetiology in northern Italy. Michele et al. 2006
Future temperature increases associated with climate change have the potential to increase the incidence of meningitis, due to a lengthening of the seasonal transmission period.130 130The impact of climate change on meningitis in northwest Nigeria: An assessment using CMIP5 climate model simulations. Abdussalam, A.F. et al. 2014 In addition, the increased frequency and intensity of droughts, and dust storms predicted to occur with climate change will also provide more suitable climate conditions to facilitate meningitis transmission.
Surveillance, from case detection to investigation and laboratory confirmation, is essential for the control of meningitis in order to: detect and confirm outbreaks; monitor trends; estimate disease burden; monitor the emergence of epidemic strains as well as their antibiotic resistance profile; and estimate the impact of meningitis control strategies, particularly preventive vaccination programmes.
Forecasting of outbreaks in sub-Saharan Africa can be achieved by using wind and dust conditions as predictors of the disease. In Niger, dust and wind conditions, combined with information on the amount of cases during the pre-season months, enable predictions of seasonal cases of meningitis.131 131Soil dust aerosols and wind as predictors of seasonal meningitis incidence in Niger. Pérez García-Pando et al., 2014
Vaccination is the main way of managing meningitis and licensed vaccines against meningococcal disease have been available for more than 40 years. However there is no universal vaccine against meningococcal disease, and each vaccine is specific to a particular serogroup. Polysaccharide vaccines are typically used during an outbreak response in Africa and offer three-year protection. A preventative vaccination strategy, involving a conjugate vaccine against N. meningitidis serogroup A that confers longer-lasting immunity is being implemented in high risk countries in sub-Saharan Africa. This offers great potential to eliminate large meningitis outbreaks as a public health problem, although reactive vaccination approaches are still an important part of the control strategy.
Chemoprophylaxis is recommended in the African meningitis belt in non-epidemic situations, and when given promptly can reduce transmission of the disease.

COVID-19 is an infectious disease, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which was first identified in Wuhan, China in December 2019. Since then, the virus has rapidly spread on a global scale, leading to an ongoing pandemic.
Most people infected with COVID-19 will experience mild to moderate respiratory illness and recover without requiring special treatment. Elderly people and those with underlying medical conditions – including cardiovascular disease, diabetes, chronic respiratory disease and cancer – are at increased risk for serious illness and death.
The potential influence of weather and air pollution on SARS-CoV-2 transmission and COVID-19 severity is an active area of research. To date, findings on the potential impact of weather conditions on COVID-19 dynamics are mixed, with no clear consensus on the direction and magnitude of the effect of meteorological and air quality factors on COVID-19.132 132First Report of the WMO COVID-19 Task Team on Meteorological and Air Quality (MAQ) factors affecting the COVID-19 pandemic. WMO 2021
Based on knowledge of other respiratory viral infections, we know that the environment may affect the spread of the COVID-19 by impacting virus survival, the human immune system, and weather-sensitive human behaviour.133 133Seasonality of Respiratory Viral Infections. Moriyama,, Hugentobler,, Iwasaki, 2020
The main routes of COVID-19 transmission include contact transmission, droplet transmission and airborne transmission.134 134Scientific Brief: SARS-CoV-2 and Potential Airborne Transmission. CDC, 2020
To date, there is no clear evidence on the influence of meteorological and air quality factors on disease transmission, suggesting that COVID-19 dynamics have been controlled primarily by government interventions rather than weather.135 135First Report of the WMO COVID-19 Task Team on Meteorological and Air Quality (MAQ) factors affecting the COVID-19 pandemic. WMO 2021
COVID-19 is an infectious disease caused by the SARS Coronavirus 2 (SARS CoC2), a virus first identified in human populations in late 2019. Transmission occurs through droplets containing infectious virus, either by direct face to face contact (splash) generated by speaking, singing, coughing or sneezing; or by aerosolisation for up to 1 metre. Virus-containing aerosols that travel further than 1 metre are defined as airborne. The virus is thought to infect humans through the mucus membranes of the eyes, nose and mouth. Living virus has been isolated from faeces and urine but neither is thought to represent a major means of transmission. Fomites are thought to represent a low risk of transmission, but the risk has not yet been quantified. The risk of transmission is greatest in closed, poorly ventilated spaces where humans are in close proximity for ten to fifteen minutes and do not physically distance or wear a protective face covering.136 136WHO 2020 via UNDRR/ISC Hazard Information Profiles: Supplement to UNDRR-ISC Hazard Definition & Classification Review: Technical Report
View more hazard definitions in our glossary >
Since the novel virus emerged in 2019, it quickly spread across the globe with sustained local transmission occurring to date in almost all countries. Transmission dynamics continue to change and evolve quickly.
Individuals infected with COVID-19 experience a wide range of symptoms, ranging from mild symptoms to severe illness. Symptoms may appear 2-14 days after exposure to the virus. Common symptoms include:137 137Symptoms of Coronavirus. CDC, 2020
COVID-19 is spread through contact, droplet and airborne transmission. The virus can spread from an infected person’s mouth or nose in small liquid particles when they cough, sneeze, speak, sing or breathe. These particles range from larger respiratory droplets to smaller aerosols.
Current evidence suggests that the virus spreads mainly between people who are in close contact with each other, typically within 1 metre (short-range). A person can be infected when aerosols or droplets containing the virus are inhaled or come directly into contact with the eyes, nose, or mouth. The virus can also spread in poorly ventilated and/or crowded indoor settings, where people tend to spend longer periods of time. This is because aerosols remain suspended in the air or travel farther than 1 metre (long-range).
People may also become infected by touching surfaces that have been contaminated by the virus when touching their eyes, nose or mouth without cleaning their hands.
Further research is ongoing to better understand the spread of the virus and which settings are most risky and why. Research is also under way to study virus variants that are emerging and why some are more transmissible.
Risk for severe COVID-19 complications increases with age, with elderly people being at highest risk. In addition, individuals of any age with certain underlying medical conditions are at increased risk for severe illness from COVID-19.138 138CDC: COVID-19: People at Increased Risk These conditions include:
There is currently no conclusive evidence that either weather or climate have a strong influence on transmission. The SARS-CoV-2 virus which causes COVID-19 disease has been transmitted in all regions of the world, from cold and dry, to hot and humid climates, and the effect of temperature and humidity in virus transmission is likely small compared to the degree of contact between people. Vaccination, physical distancing and washing hands are therefore essential to breaking the chain of transmission, and are the most effective way to protect yourself, in all locations and all seasons of the year.
Understanding the underlying mechanisms that may drive COVID-19 seasonality remains challenging due to the limited availability of accurate COVID-19 data at fine spatial scales and long time periods. Other COVID-19 risk factors, such as levels of immunity, mobility patterns and population age further need to be considered to ensure that these do not modulate study findings.
For other respiratory viral infections, including influenza, the role of weather has been more extensively investigated.139 139Seasonality of Respiratory Viral Infections. Moriyama, M., Hugentobler, W.J., Iwasaki, A., 2020 Influenza and seasonal coronaviruses tend to peak in winter in temperate regions, during colder and drier months. Temperature, humidity, ultraviolet radiation (UV) and air pollutants are assumed to be important drivers of seasonality, potentially affecting the virus viability, human resistance to infection, and human behaviour.
Direct impact on virus viability |
Controlled laboratory studies have shown that SARS-CoV-2 survives longer at low temperatures, and have yielded mixed results regarding the impact of humidity on virus stability.141 141Increasing temperature and relative humidity accelerates inactivation of SARS-CoV-2 on Surfaces. Biryukov et al. 2020; Factors affecting stability and infectivity of SARS-CoV-2. Chan, et al., 2020; The Influence of Temperature, Humidity, and Simulated Sunlight on the Infectivity of SARS-CoV-2. Dabisch et al., 2020; Experimental aerosol survival of SARS-CoV-2 in artificial saliva and tissue culture media at medium and high humidity. Smither et al. 2020 Relative humidity is assumed to modulate aerosol dynamics, potentially affecting the size and behavior of respiratory droplets, as has been shown for other viruses. In addition, ultraviolet radiation (UV) of all wavelengths, particularly UV-C radiation, can inactivate respiratory viruses under laboratory conditions. |
|---|---|
Indirect impact via host immunity |
In cold and dry settings, the body’s ability to clear virus-containing particles (mucociliary clearance) once inhaled can be impaired. Dry air may further inhibit cell repair mechanisms in the trachea and lungs.
Sudden large changes in temperature can impair the human immune system and trigger immune evasion.
Exposure to high ambient temperature, such as during a heatwave, can increase the risk of respiratory and cardiovascular diseases, in particular for vulnerable population groups. Heat-vulnerable population groups might therefore experience a higher risk of respiratory virus infection relative to the general population.
Exposure to UV-B can increase Vitamin D levels, which might stimulate immune functions.
Acute and chronic exposure to air pollutants might lead to immune system dysregulation and inflammatory responses, increasing the likelihood of cardiovascular and respiratory diseases.
These processes have not been confirmed specifically for SARS-CoV-2 or COVID-19, but are understood to be generally applicable to respiratory viruses and their associated diseases.
|
Indirect impact via human behavior |
People tend to spend more time indoors when it is particularly hot, cold and/or raining outside. Transmission therefore occurs predominantly in indoor spaces during winter months in temperate climates.
In indoor environments, characteristics of ventilation and air conditioning, such as the direction of airflow, are assumed to affect transmission rates.
Seasonality might further depend on school calendars given that school closure was found to substantially impact influenza transmission. However, the role of schools in driving COVID-19 dynamics still needs to be better understood.
|
More generally, the changing climate can contribute to pandemics by changing to habitats of animals, which can create opportunities for pathogens to jump from animals to new hosts, while many root causes of climate change, such as deforestation and land-use change, may also increase the risk of pandemics.140 140Changing rapid weather variability increases influenza epidemic risk in a warming climate. Liu et al. 2020


Research
EN
Research
EN
Research
EN